Knowledge Center
April 11, 2022
Electrosurgery: What is it, How does it Work, and What are the Benefits?
What is electrosurgery used for?

The term electrosurgery refers to the use of high frequency, alternating electric current to produce heating in tissue. The heating can be used to achieve a desired tissue effect such as cutting, tissue ablation, desiccation, or a combination of effects.1 Electrosurgical units are commonly used in Gastroenterology, General Surgery, Ob-Gyn, ENT, Pulmonary Medicine, and Dermatology, to name a few. Electrosurgery has been used in endoscopy since the 1970s.1 Its use in gastrointestinal endoscopy includes polypectomy and tissue resection procedures, hemostasis and ablation, and biliary and pancreatic endoscopy procedures.
How Does Electrosurgery Work?
An electrosurgical system consists of an electrosurgical unit, sometimes referred to as a generator or an ESU. The active electrode, the patient, and (as needed) the dispersive electrode sometimes referred to as the grounding pad. The generator takes current from the outlet and speeds it up. At this frequency, muscles and nerves are not affected, and heat is created at the cellular level.2 The heat created is responsible for the cutting and coagulation effect that is experienced.
Electrosurgery works by cutting or coagulating tissue via a high-frequency electrical current that is generated from an electrosurgical unit or ESU. The electrical current travels through an attached device (active electrode) and creates localized heating to allow for precise cuts or coagulation of the tissue which helps to reduce the risk of bleeding. By adjusting the method, mode, and power settings (wattage), physicians can customize the unit output setting for a variety of procedures.
What is the difference between electrocautery and electrosurgery?
While sometimes used interchangeably, electrosurgery and electrocautery are unique techniques. Heating the tissue directly and producing both cutting and coagulation sets electrosurgery apart from electrocautery which can only coagulate.3 Electrosurgery units create high frequency, alternating electrical currents that pass through the tissue resulting in cutting and coagulation. By contrast, electrocautery – sometimes referred to as thermal cautery – uses a connected device with a heating element. The current never passes through the patient’s body during this procedure, but cauterizes by the passive transfer of heat from the accessory and can never produce electrosurgical cutting as it does in electrosurgery.1
What is the difference between monopolar and bipolar electrosurgery?
Electrosurgical units produce currents to cut and coagulate tissue during endoscopic procedures. Most units can support both monopolar and bipolar methods. The difference between monopolar and bipolar electrosurgery is how the electrical current travels and completes the circuit. In monopolar electrosurgery, the current passes through the connected device (active electrode) directly to the affected tissue where the desired tissue effect occurs. It then passes through the patient’s body to where a dispersive pad electrode is placed. The dispersive electrode receives the current and then transmits the energy back to the electrosurgical unit to complete the circuit.
By contrast, during bipolar procedures, the electrical current flows from the generator, and is concentrated at the treatment site by the active electrode, such as a bipolar probe. Because the active electrode delivers the current to the tissue, and returns the current through the same device, there is no need for a dispersive electrode.
Physicians utilize monopolar and bipolar methods in different situations. While monopolar electrosurgery is more frequently used, the current does pass through the patient’s body to meet the dispersive electrode. Physicians may opt for the bipolar method if the patient has implanted lifesaving devices such as a pacemaker that may be adversely impacted by the monopolar current.4,5
What are the differences between cut and coagulation?
There are several modes or settings on electrosurgical generators that can allow the physician to create a desired tissue effect. These may also be referred to as outputs. Every electrosurgery manufacturer has their own names for the different outputs, but they generally range from a cut to a soft coagulation, with blended outputs in between. By adjusting the power setting and modes within the electrosurgical unit, physicians can determine the precise cut and coagulation current needed for the procedure.2
Morris, Marcia L., Hwang, Joo Ha. Electrosurgery in Therapeutic Endoscopy. 2019:69-80.e2.
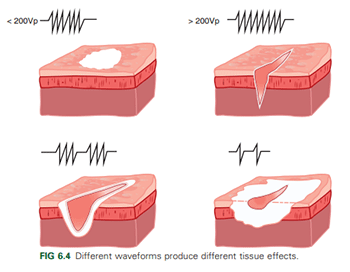
Current generated by the ESU is delivered to the tissue through accessories (active electrodes). During the application of cutting current, energy is delivered with greater intensity, promoting electrosurgical cutting.1 At the cellular level, water within the cells heats very quickly, vaporizing and causing the cell membranes to rupture. These bursting cells lead to cleavage of the tissue that lies along the accessory.1,2 This is referred to as the tissue being cut.1,2
Cells that heat more slowly dehydrate without bursting. During the application of coagulation current, energy is delivered with less intensity and promotes coagulation and desiccation.2 Coagulation current causes cell protein to denature and cells to shrink.2 Water content becomes lower, and tissue becomes more resistant to energy flow.2
The percentage of cells that burst and coagulate, as well as the amount of tissue involved, is referred to as the tissue effect.1 Although the final tissue effect seen is the result of both non-ESU and ESU variables, current density is the defining variable in determining specific tissue effects in electrosurgery.1 Variables that can affect the tissue outcome include patient information, circuit and tissue impedance, amount of tissue and the accessories involved, technique of the physician, and the time of electrosurgery application.1
What are the benefits of Electrosurgery?
Electrosurgery provides numerous benefits including but not limited to:
- Minimizes bleeding at the application
- Allows for greater precision with cutting and coagulation settings
- Offers a relatively fast method for tissue resection or ablation
What safety precautions need to be considered with electrosurgery?
As with any endoscopic procedure device, users must read and understand the operating manual provided with the device. Precautions should be reviewed to ensure safety of patient and staff. Physicians must have a clear understanding of the fundamentals of electrosurgery and the ability to adjust the settings on the device based on the clinical situation. In addition, the physician should always consider what electrosurgical accessories will be used, including snares, knives, sphincterotomes and coagulation probes.
Additional safety precautions to avoid any patient complications with electrosurgery include (not a complete list):
- Start on the lowest possible setting to avoid any unnecessary current delivery.
- Do not utilize the electrosurgical device in close proximity or direct contact with another endoscopic devices or implanted life sustaining medical devices.
- Proper dispersive electrode (grounding pad) placement is important to evenly disperse the energy and avoid any increase in skin temperature under the pad during procedures.1
- Ensure the active accessories and patient/user are not contacting grounded metal objects.
- Stay up-to-date on preventive maintenance and inspections for equipment to avoid unnecessary downtime and user or patient injuries.
Types of Electrosurgery Devices/Instruments
Common electrosurgery devices include:

- Electrosurgical unit – This device is what generates the electrical current. The gi4000 Electrosurgery Unit features a touchscreen and provides physicians with four methods designed for flexible endoscopy including argon plasma, bipolar coag, monopolar, and lavage functions.
- Dispersive electrodes, sensing and non-sensing.
- Active electrodes: there are many accessories that are commonly used in GI endoscopy procedures such as: snares, probes, forceps, knives, sphincterotomes, and many more
Contributors to this article
Gerald Chiappone, BSN, RN, CGRN
Jennifer Bailey, BS, MBA
References
1 Morris, Marcia L., Hwang, Joo Ha. Electrosurgery in Therapeutic Endoscopy. 2019:69-80.e2.
2 ASGE Technical Status Evaluation Report. Electrosurgical Generators
3 Marcia L. Morris , MS , Robert D. Tucker , PhD, MD , Todd H. Baron , MD and Louis M. Wong Kee Song , MD Electrosurgery in Gastrointestinal Endoscopy: Principles to Practice. nature publishing group
4 https://atltechnology.com/blog/electrocautery-bipolar-vs-monopolar/
5 Taheri A, Mansoori P, Sandoval LF, Feldman SR, Pearce D, Williford PM. Electrosurgery: part I. Basics and principles. J Am Acad Dermatol. 2014 Apr;70(4):591.e1-591.e14. doi: 10.1016/j.jaad.2013.09.056. PMID: 24629361.

| FOLLOW US | |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|